Prevalence and management of CVD risk factors in European patients
In 2015, just under 11.3 million Europeans had CVD leading to 4 million deaths and costing the EU economy €210 billion a year [1,2]. Most of these deaths were accelerated due to poor management of CVD risk factors such as weight, smoking and exercise.
A team from The European Society of Cardiology (ESC) led by Dr. Kornelia Kotseva evaluated guideline implementation for patients with CVD. To do this, 16,426 CVD patients from 24 European countries were surveyed 6 months following a cardiovascular event to identify risk factors, patient lifestyle, and therapeutic management. This study aimed to objectively assess clinicians’ implementation of scientific knowledge.
Surveyed patients had their obesity status measured via BMI (≥30 kg/m^2) alongside their waist circumference (F: M ≥88: ≥102 cm). Smokers could self-report as smokers or persistent smokers (smoking 1 month before a cardiovascular event). Additionally, patients had their breath CO and blood pressure measured to identify their smoking and hypertension status. Venous fasting blood samples were also taken measuring cholesterol (triglycerides, LDL & HDL) and HbA1c levels. Finally, patients were interviewed to assess physical activity levels, advising vigorous activity ≥20 minutes per week. Patients who were not interviewed had their discharge letters and medical records reviewed to retrieve data.
Three-quarters (73.55%) of CVD patients were men. Figure 1 shows the prevalence of risk factors from interviewed CVD patients. From this data, we see that healthcare professionals (HCPs) need to tackle many risk factors including the number of patients still overweight, by increasing their weekly exercise. HCPs also need to reduce lipid levels amongst CVD patients

This study has many implications for the way how clinicians across Europe manage CVD. A high proportion of patients are not meeting lifestyle, risk factor or therapeutic targets set in the JES guidelines which need to be addressed by HCPs. Studies have shown that cutting smoking reduces an individual’s risk of coronary-related mortality by 36–46% [4,5]. Despite that, less than 1 in 5 were advised to attend a smoking cessation clinic (18.1%) or prescribed nicotine replacement therapy (NRT) (14.4%) or varenicline (3.1%) — a drug shown to lead to abstinence in 51% of smokers within 16 weeks [6].
Other studies have shown the benefit of an active lifestyle alongside a good diet can bring to CVD patients. Not only have diet and exercise been shown to improve patient blood pressure, cholesterol levels, and glucose control [7,8,9], but it has also been shown to reduce patient risk of cardiovascular events [10]. However, 81.5% of surveyed patients had a BMI above 25kg/m^2. HCPs should provide patients with professional advice to improve their diet and physical activity.
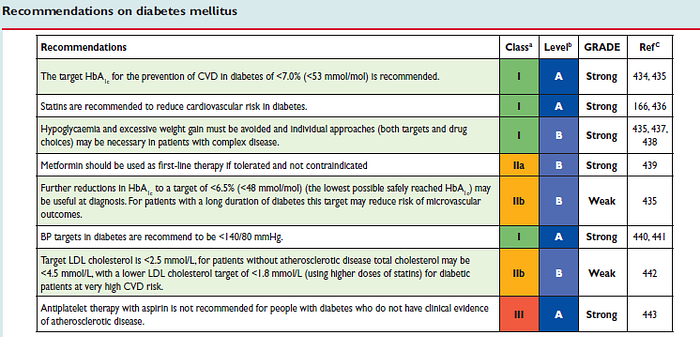
Regarding therapeutic targets, HCPs should follow the JES guidelines for cardioprotective managing their cholesterol, blood pressure, and diabetes. The study also mentioned that patients could miss biochemistry targets is due to a failure of Drs. not up-titrating therapeutic doses or beginning combination therapy. HCPs should also be reminded to engage with patients regarding medication to improve adherence and health outcomes [11].


HCPs may already be aware of guidelines and recommended practices. However, more must be done to inform patients of their health status and optimise their management plan.
1. Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, Burns R, Rayner M, Townsend N, (2017). European Cardiovascular Disease Statistics 2017. European Heart Network, Brussels.
2. Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37(42):3232–3245. doi:10.1093/eurheartj/ehw334
3. Kotseva K, Wood D, De Bacquer D et al. EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur J Prev Cardiol. 2015;23(6):636–648. doi:10.1177/2047487315569401 — Article source
4. Critchley J, Capewell S. Mortality Risk Reduction Associated With Smoking Cessation in Patients With Coronary Heart Disease. JAMA. 2003;290(1):86. doi:10.1001/jama.290.1.86
5. Wilson K, Gibson N, Willan A, Cook D. Effect of Smoking Cessation on Mortality After Myocardial Infarction. Arch Intern Med. 2000;160(7):939. doi:10.1001/archinte.160.7.939
6. Jennings C, Kotseva K, De Bacquer D et al. Effectiveness of a preventive cardiology programme for high CVD risk persistent smokers: the EUROACTION PLUS varenicline trial. Eur Heart J. 2014;35(21):1411–1420. doi:10.1093/eurheartj/ehu051
7. Carpio-Rivera E, Moncada-Jiménez J, Salazar-Rojas W, Solera-Herrera A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq Bras Cardiol. 2016. doi:10.5935/abc.20160064
8. Mann S, Beedie C, Jimenez A. Differential Effects of Aerobic Exercise, Resistance Training and Combined Exercise Modalities on Cholesterol and the Lipid Profile: Review, Synthesis and Recommendations. Sports Medicine. 2013;44(2):211–221. doi:10.1007/s40279–013–0110–5
9. Yan H, Prista A, Ranadive S et al. Effect of Aerobic Training on Glucose Control and Blood Pressure in T2DDM East African Males. ISRN Endocrinol. 2014;2014:1–6. doi:10.1155/2014/864897
10. Agarwal S. Cardiovascular benefits of exercise. Int J Gen Med. 2012:541. doi:10.2147/ijgm.s30113
11. Dang B, Westbrook R, Njue S, Giordano T. Building trust and rapport early in the new doctor-patient relationship: a longitudinal qualitative study. BMC Med Educ. 2017;17(1). doi:10.1186/s12909–017–0868–5
12. Perk J, De Backer G, Gohlke H et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) * Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2012;33(13):1635–1701. doi:10.1093/eurheartj/ehs092
